

On 28 August 2023 at 0844, N109BC, an EC135 T1 helicopter, crashed in Pampano Beach, Florida killing Captain Terryson Jackson, a paramedic in the aircraft, and one person on the ground. The other paramedic and the pilot were injured and 2 other people on the ground were also injured. The accident report was released by the NTSB on 11 September 2025 and concluded that the cause was:
“An inflight fire outside of the engine firewalls, likely from overheating of the No. 1 engine for undetermined reasons, which resulted in a partial tailboom separation.”
NTSB Final Report – ERA23FA352 – NTSB
Report omissions
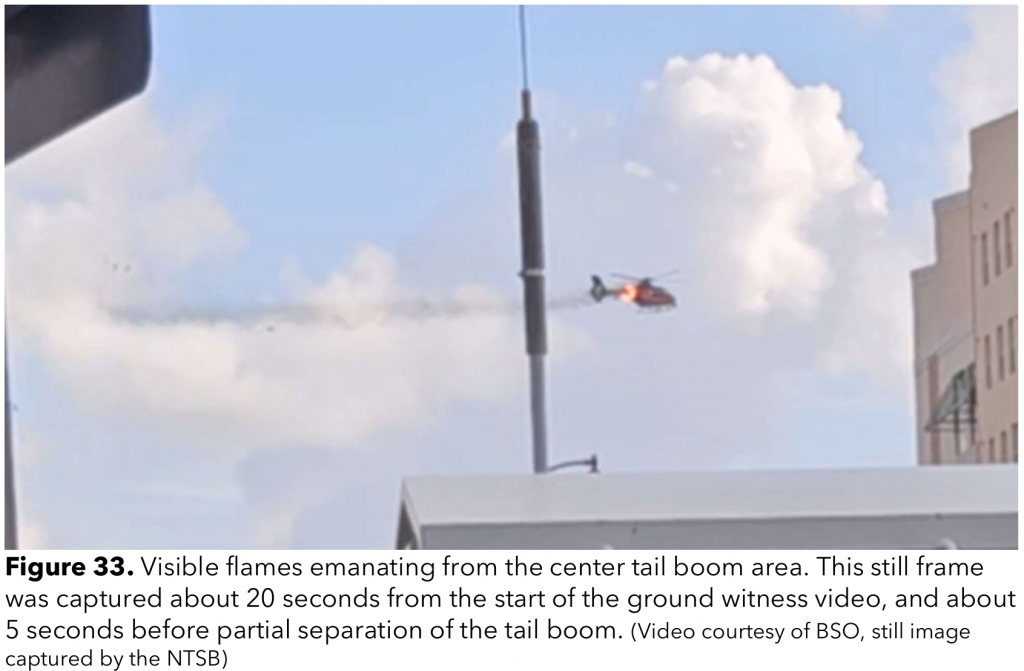
That is indeed the direct cause of the crash. It could be argued that could have been concluded very quickly just based on the videos that circulated (see example below). It is quite disappointing that the NTSB then do not go on to explain why the fire got to the point of severing the tailboom before the aircraft landed and how the situation could be prevented in the future. For comparison, look at the detailed conclusions in the AAIB report on the G-SPAO accident where an EC135 crashed into a building (AAIB)
There are also no safety findings in the NTSB’s report. The team over at Pilots Who Ask Why did a great analysis of the report (see link below) and added some lessons learned on the basis of the report. But this still leaves many questions un-answered. Pilots Who Ask Why
This prompted a review of the NTSB report and it is immediately obvious something is not right. Some of the EC135 terminology used in the report is wrong and there some glaring omissions in the scope of the investigation. For reference, the investigation was a Class 3 investigation (Aviation Investigation Classification). The big investigations are Class 1. A broader and deeper dive into the NTSB docket for incident revealed some worrying omissions that need to be discussed in deeper detail. The docket is here: NTSB
Let’s dig in
Incident summary
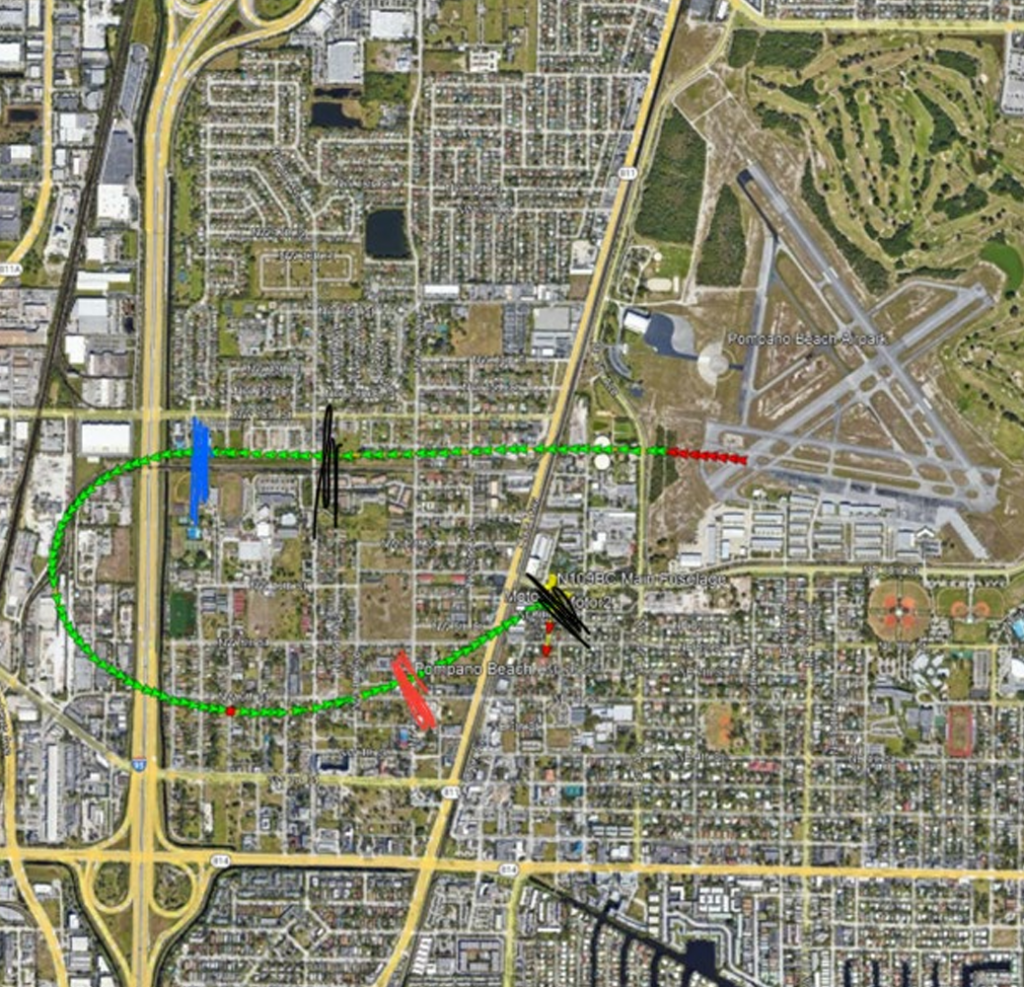
The incident occurred during a callout of the helicopter to an incident in North Lauderdale, which came in as the crew were checking the aircraft ready for the shift. The crew grabbed their equipment and launched south west bound from Pampano Beach Airpark.
Just after the pilot left the airport frequency, things went wrong. The crew heard a loud bang and the pilot noted a rising Turbine Outlet Temperature (TOT) on the No 1 engine. He put the No 1 engine to IDLE using the engine switch and initiated a return to the airfield 2 miles behind him. During the flight back to the airfield, the FIRE light and audio came on. Subsequently, the tailboom detached and the aircraft crashed into a residential building roof. The aircraft was airborne for less than 3 minutes.
The aircraft
N109BC was an EC135 T1 and was built in 1999. This is a very early model EC135 with serial number 0139. It was equipped with analogue instruments and a CDS (Cockpit Display System) panel and was not IFR capable.

{kind=link}
Engines
The aircraft was equipped with 2 Arrius 2B1 FADEC controlled-engines which were equipped with a fire suppression system with one bottle which could discharge into either engine. The engine was surrounded by a titanium firewall. In the event of FADEC failure, the engine could be controlled by two collective-mounted throttle twist grips.
Of note, unlike most later EC135, the engine was not fitted with an overspeed protection system (see NTSB Powerplant Group’s report here: NTSB)

Cockpit displays
The CDS is an early version of the CPDS which might be more familiar to EC135 pilots – no FLI here. It has a caution display at the top and a digital LCD display of data at the bottom. If a caution illuminates on the caution display a caution button also illuminates but there is no audio (nor is there audio for cautions on EC135 CPDS).
The pilot can also get engine performance and health data from some analogue gauges. If a red warning light illuminates on the fire panel there is an associated “bong” audio which repeats until acknowledged. If there is a fire warning, a repetitive “ding, ding, ding…” audio sounds until the fire is extinguished. For the fire bottle to fire, the engine N1 needs to be below 50% and the FIRE light must be illuminated.
Dependent on if a modification is embodied (SB 135-26-006) the relevant EMER OFF switch needs to be pressed as well. This was embodied to stop inadvertent fire bottle firing. It is unknown whether this was embodied on this aircraft. The EMER OFF switches activate the emergency fuel shut off to the engines no matter what the modification state of the aircraft.

Engine Controls
The aircraft had a pair of manual throttles as twist grips on the collective. They are called twist grips by Airbus and pilots of the EC135 as moving them illuminates the TWIST GRIP caution. These allow manual control on the engine speed when the FADEC stops working or behaves abnormally. This is automatic if the FADEC FAIL caution occurs or the engine can be selected into manual by the pilot moving a switch on the overhead console. The engines can be shut down completely if the throttle is fully rotated to minimum, the idle stop is released and twist grip moved all the way to off.

The engines are normally controlled by the pilot moving the yellow engine switches on a panel to the right of the CDS.

Additional equipment
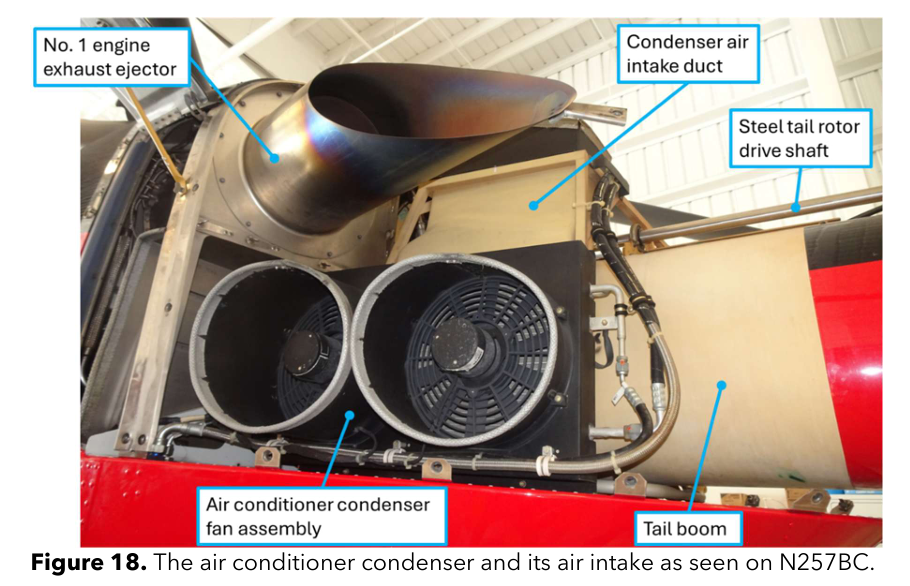
The relevant extra kit on the aircraft was an air conditioning system mounted aft of the left engine.
The pilot
The NTSB docket documents contains a lot of information about the pilot (perhaps too much – his name is not redacted). He had a lot of experience in general (4035 hrs) and a substantial amount on the EC135 (272 hrs). It is not however recorded how much of that is on the T1 CDS variant. It highlights no issues with his qualifications or currency to operate. There is very little recorded about his training except his last check ride was on 9 June 2023, two months previously.
He was interviewed by police less than 4 hours after the accident having just lost a close colleague in the seat next to him
He gave a pretty full account of the incident as did the paramedic seated in the rear cabin. NTSB
The pilot answered some further questions a few months later NTSB
The pilot answers some NTSB questions by phone the following year NTSB
The pilot reported his recollections, his decision making process and what he thought had occurred. As with any testimony taken in the immediate aftermath of a traumatic event, there are inconsistencies with the evidence (eg the activation or not of the EMER OFF switch) but that is up to the investigators. I salute the pilot for being able to hold it together just 4 hours on from a brush with death.
The report
Mistakes and errors
So with the background set out, the report should bring together all the detailed information in the many documents in the docket in an easy to digest form. However, following a review of the report and the associated documents, some worrying issues arise.
Throttles and switches
Reporting error
The final report states:
“He set the No.1 engine throttle to idle, declared an emergency to air traffic control, and reversed direction to return to the airport. Unbeknownst to the pilot, due to the FADEC FAIL condition, setting the engine throttle to idle would have had no effect on fuel flow, but rather the engine twist grip would need to be manipulated to manually control fuel flow to that engine.”
For the EC135 pilots in the room, they will scratching their heads. The twist grips are the throttles on an EC135. What does the pilot mean? Well actually, the pilot never said he put the throttles to idle in any of the 3 documented interviews. He even clarified in the second written statement: “I used my left hand, verified the switch, removed the “Flight” Guard, put it to idle, announced to the crew what I was doing.
This was done by Engine Switch, not throttle or manual mode.” The use of the word “throttles” in this case is an NTSB error. He stated he never saw the FADEC FAIL caution as the engine froze, but it could not be proven either way whether it did actually get displayed on the CDS (the CDS memory could not be downloaded).
What the pilot saw
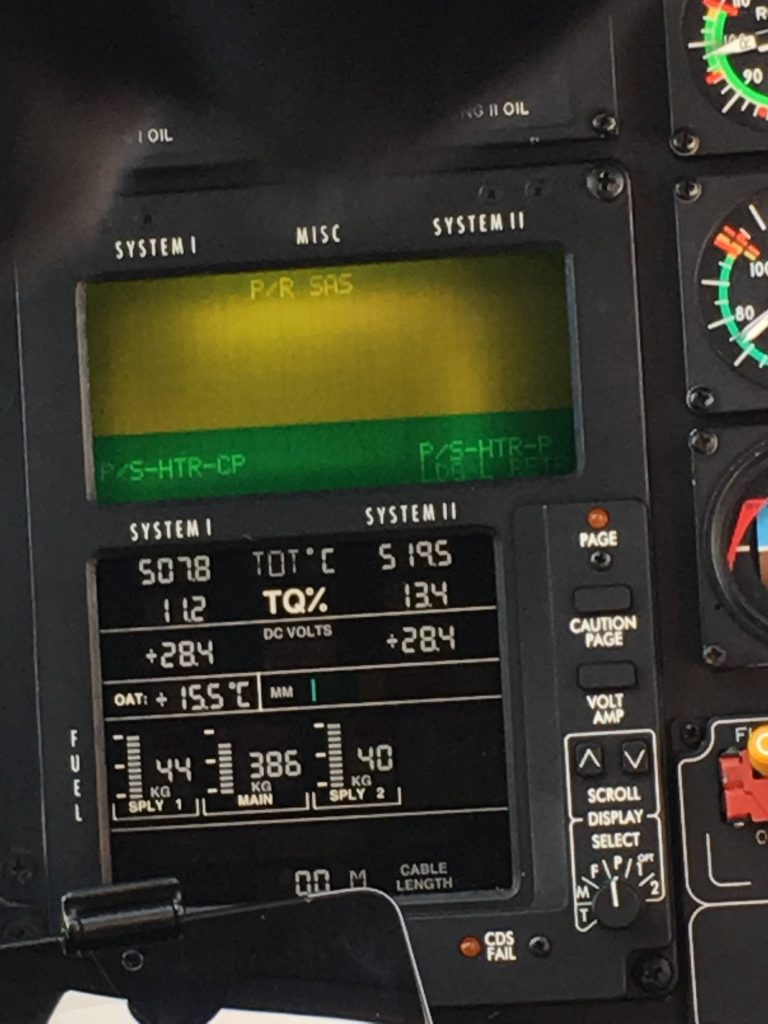
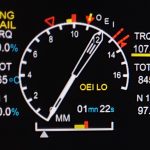
Now that is established, let us break down what he saw to lead him to make that switch selection. The pilot stated that after the first bang, 90 seconds after take off, that he looked at engine gauges and noticed a high TOT which was rising. TOT is not normally shown on the CDS so he must have been looking at the TOT dial. This has one needle per engine, which routinely close together with a small 1 or 2 on them – hard to see in the image below.

What the pilot did
There is no emergency procedure for a high TOT, but perhaps following a loud bang and an abnormal TOT indication, that the engine is not performing well and its reasonable to begin the engine failure procedure. The procedure in the Airbus checklist and Flight Manual is a memory drill (written in bold):
Procedure:
- OEI flight condition – Establish
- Affected engine – Identify
- Single engine emergency shutdown – Perform
- Land as soon as practicable
The pilot did get the aircraft in an OEI condition (defined in the pilot checklist) and he did correctly identify the failing engine. However, the single engine emergency shutdown is:
Procedure:
- ENG MAIN sw (affected engine) – OFF
- If cause is not mechanical…engine ventilation – Perform
- Respective twist grip – Turn to min stop, verify correct engine then shut off
So, the correct procedure is to switch the engine OFF. The procedure does not mention stopping at the IDLE position first. However, this is absolutely the right thing to do to check to ensure you are moving the right one. Unfortunately, the pilot removed their hand from the switch and then stated they did not shut it down because they feared shutting down the wrong one based on other accidents. There was very little risk of doing so, as the switch in the IDLE position is visually obvious and the guard would have still been in place on the other engine.

It is also worthy of note, that should the engine keep running, as was the case here, the twist grip should be moved to shut off. This did not happen.
In conclusion, the pilot never fully actioned the engine shutdown procedure in accordance with the emergency procedure due to a fear of inadvertently shutting the wrong engine down.
Engine fire procedure
Reporting Error
In the final report, the NTSB highlight that the EMER OFF switch was not pressed and the emergency fuel shut off was not closed. The pilot however stated on three occasions they pressed the button. In addition the pilot states they saw the green “ACTIVE” indication. On this point, the NTSB did some excellent technical analysis of the systems.
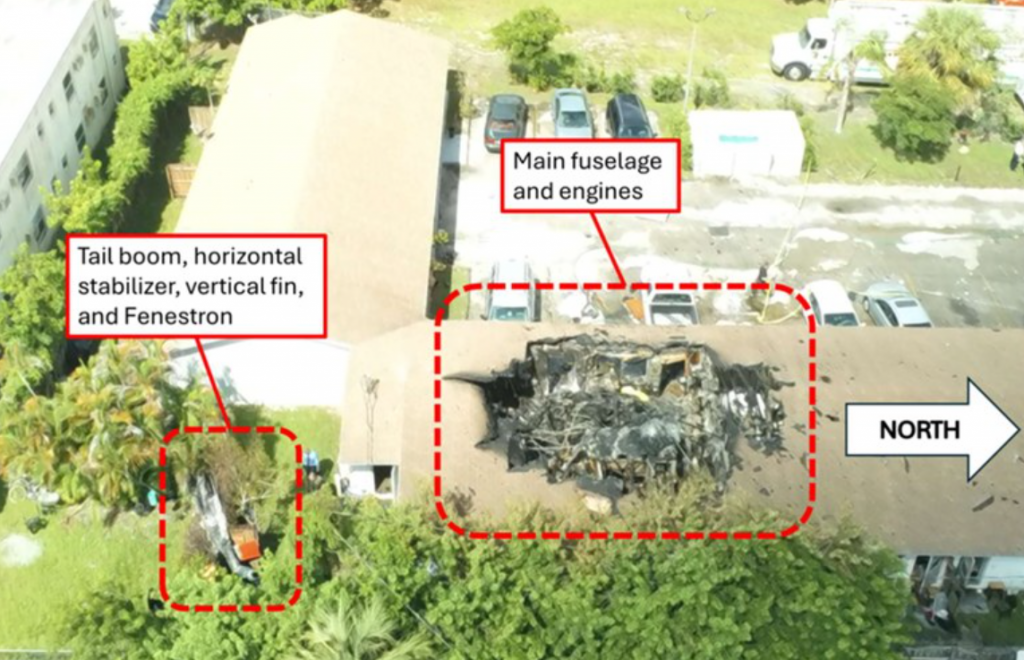
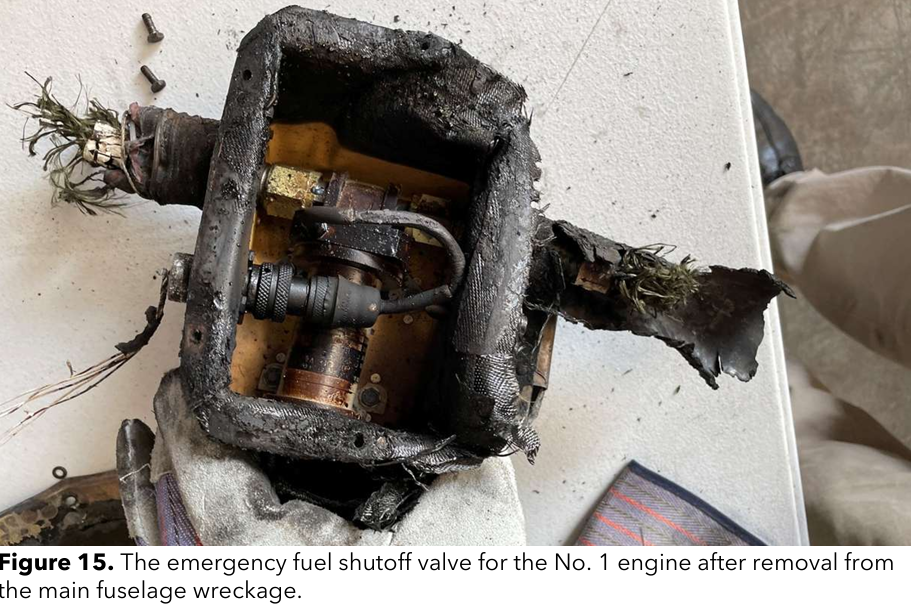
As can be seen from the post accident wreckage inspection, the investigators did a deep technical analysis of the EMER OFF sw and shut off valve to determine their position (see the Airworthiness Group report). As can been seen from the images below, there was substantial fire damage to the fuselage and yet the investigators made a great job of technically analysing the components to determine their position.

With that excellent analysis in mind, it is quite worrying to read the description of the fire suppression system in the aircraft:
When a fire is detected within the engine compartment, the engine fire light on
the warning unit illuminates and an aural tone that is unique for engine fires will
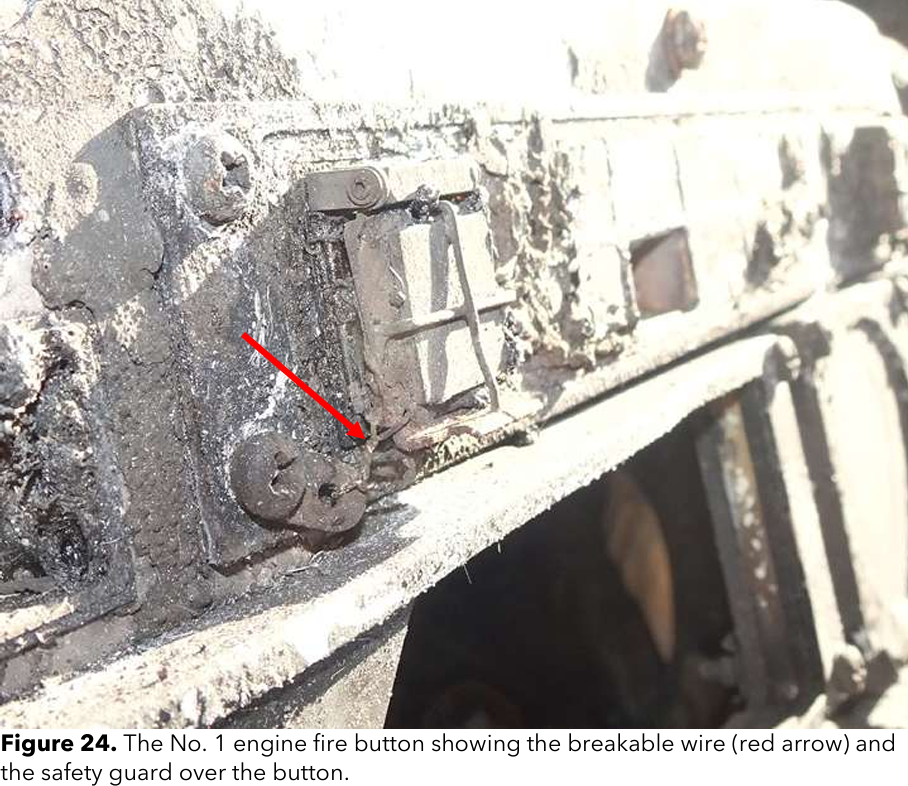
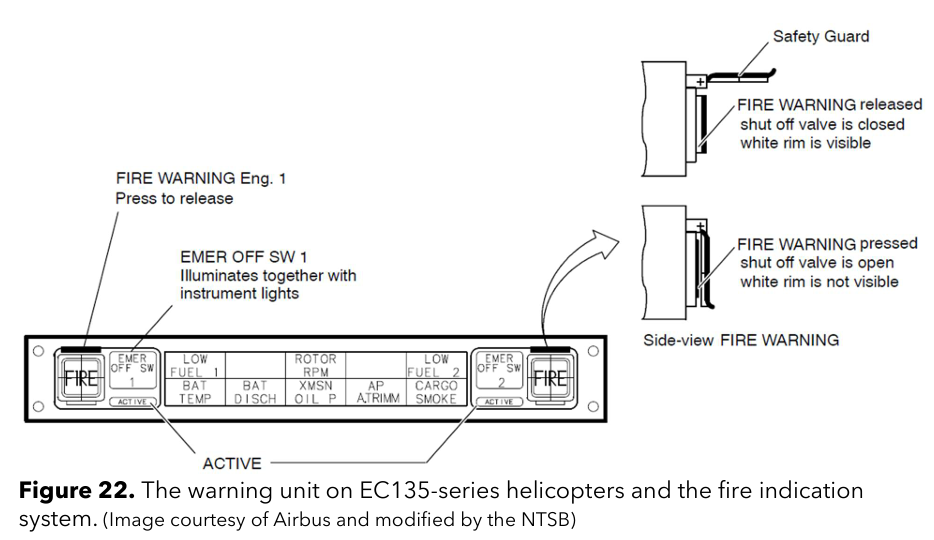
annunciate. To activate the engine fire extinguishing system, the engine fire button’s safety guard needs to be opened in order to press the engine fire button (Figure 22). The safety guard is a protective grill that covers the engine fire button. A breakable wire is affixed to each safety guard to prevent inadvertent opening of this safety guard, but also to allow for breaking the wire to open the safety guard in an emergency. Once the fire button is pushed, the engine fire button will extend, revealing a white border on the outer perimeter of the button. The engine’s emergency fuel shutoff valve closes, illuminating the “EMER OFF SW” light next to the engine fire button that was pushed. The fire extinguishing system is armed until the respective engine gas generator speed (N1 or Ng) decreases to below 60%, at which time the fire extinguishing agent is released into the respective engine compartment. When the fire extinguishing agent is released, the light labelled “ACTIVE” will illuminate next to the engine fire button that was pushed.
OK let us unpack the 4 major errors here:
- On early EC135 like this one, the only 2 things that had to happen for fire extinguisher release were 50% N1 and an illuminated FIRE light. The requirement for the button to be pressed as well was only added with the optional SB 135-26-006. There is no indication this modification was embodied and it was only recommended not mandatory so it is probably unlikely. Had the pilot shut down the engine, the fire extinguisher probably would have fired, even though the EMER OFF switch was not pressed.
- The EMER OFF caption does not illuminate when the button is pressed. The EMER OFF caption is backlighting that is linked to general cockpit backlighting.
- The fire extinguisher will not discharge until 50% N1 not 60% as stated.
- The ACTIVE green light illuminates when the EMER OFF switch is released, not when the extinguisher fires. On a CDS cockpit, there is no indication the fire bottle has discharged For later model EC135 pilots, there is no FIRE EXT caution on CDS.
So overall, very poor accuracy from the NTSB on this topic. In any case, lets look at what the pilot saw and did next.
What the pilot saw and heard
The pilot stated they saw the illuminated FIRE button and the associated “ding, ding…” audio. That is a clear indication of an engine compartment fire. Or is it? As the NTSB correctly highlight, it is an indication of a high temperature in the engine compartment. The pilot also stated in a later interview that simultaneously he saw a HTG OVTEMP caution. One of the sensors for this is between the 2 engine bays. Thus, it may have been very hot rather than a fire. Nevertheless, pilots are trained to react to such situations as a fire.
What the pilot did
The procedure is:
Procedure:
- Collective lever – Adjust as necessary to prevent the normal engine from overloading when affected engine is cut off.
- Respective EMER OFF sw – Open switch guard, press and release
NOTE: Respective engine will automatically cut off “ACTIVE” will illuminate on the EMER OFF sw panel and F VALVE CL will illuminate on the CDS
3. Affected engine – Identify
4. Single engine emergency shutdown – Perform
5. Passengers – Alert
If FIRE WARNING is OFF:
6. LAND AS SOON AS POSSIBLE
If FIRE WARNING remains on:
6. LAND IMMEDIATELY
The pilot stated they pressed the fire button several times. However, it was found to have never been pressed. The pilot stated at the first interview that they saw the green ACTIVE light. This is extremely unlikely as it is only illuminated when the guard is raised and the switch pressed and released. Whilst it is understandable that the pilot mis-remembered such a traumatic event, it does raise a question about whether he saw an earlier FADEC FAIL caption – we will look at this in a moment.
What we can say, is the pilot never actually actioned the fire procedure. Even had he pressed the EMER OFF sw, he also did not shut the engine down as in the procedure. Finally, he did not “land immediately” as required for an unextinguished fire. That last point however, I can sympathise with. He had very limited options below and he had the airfield 30 seconds in front of him. The NTSB probed his decision making in the third interview, but the pilot stated an immediate landing would have been reckless. I have to agree – see the image below.
In conclusion, the pilot again did not fully action the fire emergency procedure by shutting the engine down, although he was understandably focused on setting up for landing.
Report Omissions
Now lets look at what was missed by the reporting. The NTSB team did a detailed deep dive into the technical aspects of the incident but did not dig into the training or operational background.
Audio Gongs
On several occasions during his second interview, the pilot mentioned not hearing audio “gongs” when cautions appeared:
“He stated that he did not hear the aural gong (for caution indications) at any time, and that the HTG OVTMP indication could have triggered the aural gong…”
“He stated he does not distinctly remember hearing the aural gong (for caution
NTSB
indications) annunciate during the accident flight.”
The NTSB do not seem to have picked up on this and queried this further. On EC135 there is no audio alert associated with a caution message. Digging deeper here may have uncovered more detail about the pilots training. Had he have experienced a simulator environment with cautions being generated during emergencies, he would likely have known that cautions have no audio and that vigilance is required by the pilot to catch messages on the CDS.
FADEC FAIL / Governor Malfunction
Early in the final report, it states the investigative team identified that the engine recorded an event for a level 3 FADEC malfunction. This should have generated a FADEC FAIL caution. The pilot stated he never saw such a caution. Unfortunately, whilst the CDS computer was relatively undamaged, no useful data could be extracted regarding what cautions had been displayed (see the Airworthiness Group report). What the NTSB failed to dig into was why the pilot never actioned a governor malfunction procedure which was still indicated by other displays in the cockpit.
Leaving the lack of a caution aside, the report highlighted the fuel flow stuck at 122 litres per hour on the No 1 engine. That’s 97.6 kg per hour which is full power. When the pilot lowered the collective to stop the climb, the remaining engine would have backed off, giving a TOT, N1 and torque mismatch which would have been displayed on the dials and the CDS digital N1 readout (the default CDS display is N1 for the T1 and torque for the Pratt and Whitney engined P1). Whilst the pilot under questioning could not recall what parameters other than TOT were indicating, had he done so he would have seen all the engine 1 indications were high. This should have led the pilot to action the engine overspeed – governor malfunction procedure which begins as follows:
- Collective lever – Raise to maintain N2 and NR within limits
- Affected engine – Identify
- TWIST GRIP (affected engine) – Reduce torque until the normal engine takes the load (TWIST GRIP and DEGRADE caution comes on)
- …..
The pilot never touched the twist grips, as highlighted in the report. Doing so may have brought the engine speed and temperature down and contained the emergency long enough for a safe landing.
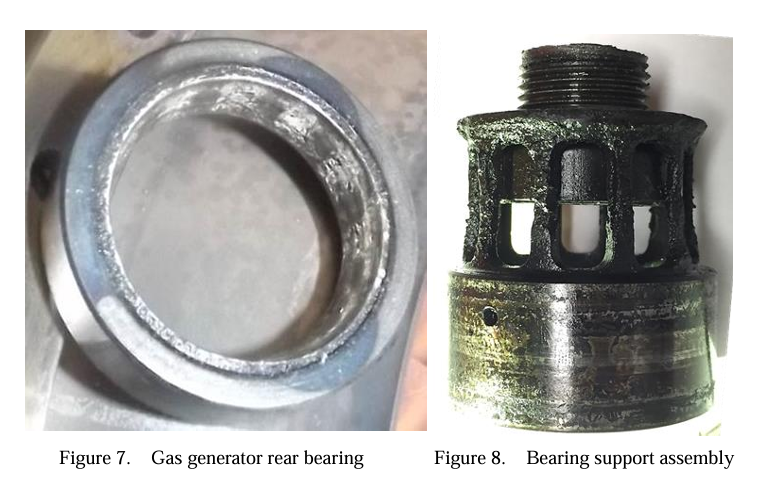
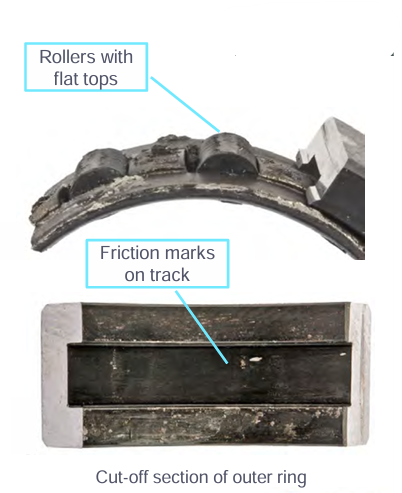
Trigger for engine overheating
Despite the extensive technical investigation of the engine, the NTSB were unable to determine a cause for the engine to overheat. Essentially the whole root cause of the engine overheating and subsequent fire has not been determined. Whilst guessing as to a cause helps no one, one possible cause does not seem to have been considered. On several occasions, the NTSB assert there was no fire inside the engine compartment; instead the fire happened at the rear of the engine in the vicinity of air conditioning ducting made of fibreglass. However, the most rearwards bearing of the engine was found to be completely disintegrated (called the Power Turbine rear thrust bearing).

This seem to have a very close match to 2 similar incidents on 2 EC145 in 2017. In these incidents, oil supply and scavenge issues, due to coking, caused in one case an engine fire and another case a rapid rise of TOT with associated FADEC failures. Whilst the NTSB did look at several power turbine blade separation events, they seem to have missed looking at events with engine fires and rapid TOT rises. It may be unrelated but, appears similar. For reference the two EC145 incidents are:
- EC145 N146DU on 8 September 2017 – High TOT, bearing failure
Previous training
The NTSB do not look into the pilots training history. The pilot did not complete any of the three potential emergency drills (engine fail, engine fire or governor malfunction). In particular, the NTSB never dig into what aircraft variant he did his initial or recurrent training in and whether the pilot had had the opportunity to fully action any of these drills. In particular, had the pilot ever actually lifted the EMER OFF guard? We are fortunate in the UK to have an FTD 3 EC135 simulator where every pilot has used this switch in anger.
There is no approved T1 CDS simulator anywhere in the USA or overseas. There is also no FAA approved EC135 simulator with an Arrius engine modelled. Of the 4 simulators approved in the USA all of them represented a Pratt and Whitney engined EC135 P2+ which in addition to have different engines, has a significantly different cockpit. The cockpit is a glass FCDS cockpit with a CPDS in place of the CDS. The nearest facility was in Louisiana but it is unknown whether the crews used this simulator and if they did, what differences training took place on the T1 CDS variant. Of particular note, the FADEC FAIL procedure is identical between T1 and P2+ but has wildly different indications due to the difference between CDS and CPDS.

In addition to the lack of commentary on the use of FSTD, the NTSB do not comment on the aircraft last used for recurrent checking. This is recorded on the accident form as a T2+. This would have the FCDS/CPDS as shown above and it is highly likely all emergencies were simulated using touch drills only. See the accident form here: NTSB
From this we cannot make any definitive safety conclusions but we can postulate that it is unlikely the accident pilot had practiced actually moving the EMER OFF switches, actually moving the engine switches in flight and actually moving the twist grips in response to a governor malfunction in flight.
It is interesting to note that there is now a very realistic simulation of an EC135 T1 CDS included with Microsoft Flight Simulator 2024. As can be see in the screenshot below, it can simulate a FADEC FAIL quite well. If the pilot had had such a non-regulated training tool, would he have been more confident in actually moving the engine switch to OFF?

Safety recommendations?
The final thing the NTSB failed to include was any safety recommendations. Several spring to mind:
Simulator training
Although there is insufficient detail in the report about the pilot’s emergency training, what is clear is that he was afraid of shutting down the wrong engine. That fear could probably have been overcome with regular practice in a simulator. Despite the variance in cockpit, the use of the EMER OFF switch in particular is identical between T1 CDS and P2+ CPDS cockpits. The NTSB should have recommended simulator training for EC135 pilots, even if it was just a desktop PC version.
Turbine blades
The report identifies that the accident aircraft’s number 1 engine had 5 power turbine blades detach. This may had been the result of the fire or the cause of it. The report further highlights that turbine blade detachment is a known issue on this version of the engine (the Arrius 2B1) and there is modification to fit upgraded turbine blades. However, at the time of the report, the Safety Bulletin mandating this upgrade gave operators 500 hours of flying or until 31 December 2026 to install the new turbine blades. The NTSB should have recommended speeding up this process.
Overspeed protection
Whilst not directly called out as a cause for this incident, the Powerplant Groups report highlights that the engine in this aircraft had no overspeed protection (which is now standard on EC135). The NTSB could not definitively say the engine didn’t overspeed at some point (which would have cause power turbine blade loss) but recommending fitment of the overspeed protection system might have been useful.
Data recording
The investigation was hampered by a lack of crashworthy data and voice recording. It is not currently mandated for the type of operation being flown in the USA but is mandated in the UK and Europe. The NTSB should be consistently recommending CVR/FDR fitment.
Conclusion
The NTSB did a fantastic job of digging into the technical aspects of this accident where 2 people lost their lives. However, the accuracy of some aspects of the report, the lack of detail regarding the pilot’s training and a complete lack of any safety recommendations leaves a lot of questions. I think the pilot did all they could given the probable lack of simulator training and opportunity to move switches during emergencies. Remember the pilot is just as much a victim of this accident as those who were killed.
I feel we have not learnt enough from this tragedy and a similar event tomorrow might have a similar outcome.
Check out my other articles…
- Keeping up with the Norwegians – Six amazing innovations for UK HEMS

- LNAV/VNAV (SBAS) – Are they approved for use in the UK?

- Helicopter 2D IFR approaches – Is CDFA the best choice?

- Understanding Helicopter Flight Manuals – Everything you need to operate safely

- Post Maintenance Flight Tests – How to avoid fatal traps

- First Limit Indicators in Helicopters – Deadly mistakes to avoid
- Bad Vibes – How to report vibrations on helicopters

- Autopilots, cross-checks and low G in helicopter unusual attitude recovery

- Expert site surveys – Improving the assessment of onshore landing areas

- Lights, helipad, action! The problem with new helicopter pad lights

- Helicopter on Fire – Could accident investigators have learned more?

- The Ultimate Medical Helicopter – Selecting the right machine for HEMS

- Deconfliction in HEMS operations – Practical methods for keeping apart

- HEMS Landing Sites – Reliable places to drop your medics

- Planning to fail – The perils of ignoring your own advice

- 2D or not 2D – How much room do I need to land a helicopter?

- What is your left hand doing? How to use a 3-axis autopilot on helicopters

- My tail rotor pitches when it flaps! Why?

Leave a Reply